Hand Numbness Is the First Sign of Nerve Damage: Carpal Tunnel Syndrome

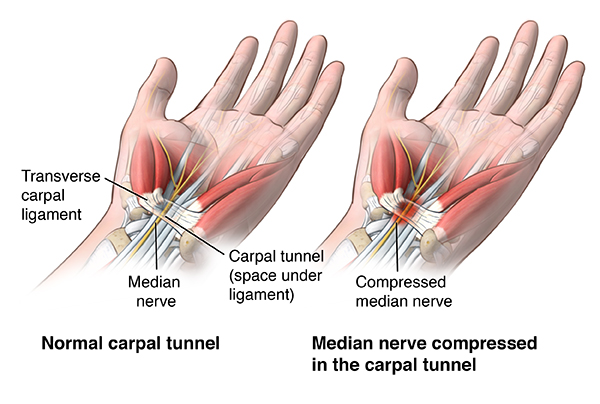
Carpal tunnel syndrome is a condition in which the median nerve is subjected to prolonged compression within the carpal tunnel at the level of the wrist. The underlying problem is not muscle inflammation, joint wear, or skin damage, but chronic pressure on the nerve within a confined anatomical space.
The median nerve is responsible for sensation in the thumb, index finger, middle finger, and the adjacent part of the ring finger, and it also participates in controlling fine hand movements and grip strength. When the conditions under which it functions are disrupted, numbness, tingling, pain, a feeling of clumsiness in the hand, and reduced precision of movements appear.
It is important to understand that in carpal tunnel syndrome the hand may appear externally healthy. The joints, tendons, and skin often remain without pronounced structural changes. Symptoms arise because the nerve that transmits signals between the hand and the brain functions for a long time under conditions of increased pressure and impaired blood supply.
Carpal tunnel syndrome is not a one-time injury. It is a process that develops gradually. As long as pressure within the carpal tunnel persists, the nerve has no opportunity to recover, even if symptoms temporarily weaken. This is why early understanding of the nature of this condition is crucial for choosing the next steps.
Why carpal tunnel syndrome develops
Carpal tunnel syndrome does not form due to a single episode of load, but as the result of a combination of factors that consistently increase pressure inside the carpal tunnel and deprive the median nerve of the ability to recover. The core of the process is prolonged nerve compression, while other factors either increase the pressure or help maintain it.
Chronic compression of the median nerve
The carpal tunnel is a rigidly confined space, the walls of which are formed by the wrist bones and the transverse carpal ligament. Unlike muscles or soft tissues, this tunnel is practically incapable of stretching. Therefore, any-even minor but persistent-increase in the volume of its contents leads to a rise in intratissue pressure.
The first consequence of prolonged pressure elevation is disruption of microcirculation within the nerve itself. The median nerve is supplied by small vessels that are sensitive to external compression. With chronic compression, venous outflow deteriorates first, followed by impairment of arterial blood supply, resulting in local ischemia of the nerve fibers. These changes may develop slowly and for a long time may not be accompanied by gross structural damage, but even at this stage conduction of nerve impulses is disturbed.
With ongoing compression, the myelin sheath of the nerve fibers, which is responsible for the speed and accuracy of signal transmission, becomes affected. Slowing of conduction initially manifests as sensory symptoms-numbness, tingling, a sensation of a “foreign hand.” If the pressure persists, motor fibers become involved, leading to reduced strength and coordination of movements.
The key factor is the duration of exposure rather than the force of a single compression episode. Short-term increases in pressure may be compensated, whereas prolonged-even moderate-compression deprives the nerve of a recovery period. As long as the pressure does not decrease, regeneration of myelin and restoration of normal conduction are impossible, even if symptoms temporarily diminish.
Repetitive loads as a factor that fixes compression
Repetitive movements maintain constant tension in the finger flexor tendons. Under conditions of repetitive or long-lasting loads, this leads to a sustained increase in pressure within the carpal tunnel and leaves the median nerve without time to recover.
Working at a computer, using a computer mouse, and using a smartphone are accompanied by prolonged fixation of the hand in a non-physiological position. When using a mouse, the wrist is often held in static extension or deviation to the side, while the fingers perform repetitive fine movements. When using a keyboard and a smartphone, flexion and extension of the wrist and repetitive finger activity are added. This combination increases pressure in the carpal tunnel and impairs fluid outflow, especially during many hours of work without breaks.
Repetitive small hand movements, even without significant force load, overload the finger flexor tendons. When such a load is constant, tendon swelling gradually develops. In the confined space of the carpal tunnel, even moderate swelling quickly affects the condition of the median nerve.
Working with hand-held and vibrating tools, as well as brush painting, creates a specific type of load. The hand is held for a long time in a state of static tension, the fingers fix the tool, movements are repeated many times, and vibration further increases the load on the tendons and the nerve. This combination contributes to an increase in intratissue pressure and to the maintenance of median nerve compression.
Force and static loads on the hands, including weight bearing on the palms, loaded grips, and prolonged weight holding, lead to a sharp increase in pressure inside the carpal tunnel. Even with good physical conditioning, regular use of such loads can maintain nerve compression.
Hand position during sleep also plays a significant role. During sleep, the wrists often involuntarily flex or hyperextend and may remain in this position for many hours. Such prolonged fixation imperceptibly maintains compression of the median nerve throughout the night, which explains the characteristic nocturnal awakenings and morning hand numbness, even if daytime symptoms are moderate.
Soft tissue swelling and fluid retention as the main factor increasing pressure
Swelling of the tendons and surrounding soft tissues leads to an increase in the volume of the contents of the carpal tunnel and to a rise in intratissue pressure. Since the tunnel is not capable of expanding, even a small increase in tissue volume affects the condition of the nerve.
Fluid retention may intensify at night, during hormonal fluctuations, and in systemic inflammation. Under such conditions, compression of the median nerve is maintained even in the absence of pronounced external load on the hand.
Metabolic and hormonal factors as the systemic background of the process
Disorders of carbohydrate metabolism promote inflammation and tissue swelling, including the structures of the carpal tunnel. Hormonal changes affect fluid retention and the condition of connective tissue.
These systemic factors are not a direct cause of carpal tunnel syndrome, but they create a background on which local compression develops more rapidly, proceeds more persistently, and responds worse to recovery. This is why, under the same load, carpal tunnel syndrome does not develop in everyone. The combination of swelling, hormonal fluctuations, metabolic features, and individual vulnerability of nervous tissue determines how quickly compression forms and how stably it is maintained. In this context, load acts as a trigger rather than the sole cause of the process.
Risk Factors and Predisposition
-
Fluid retention and tissue swelling Hormonal factors increase fluid retention and expand soft tissue volume. This is why carpal tunnel syndrome may occur temporarily during pregnancy due to pronounced fluid retention.
-
Metabolic and endocrine conditions Diabetes, thyroid disorders, and excess body weight contribute to fluid retention and changes in tissue properties, increasing pressure within the carpal tunnel and reducing the nerve’s tolerance to compression.
-
Structural tissue changes Inflammatory joint diseases (including rheumatoid processes) and degenerative changes can thicken tissues in the carpal tunnel and alter its shape, increasing pressure on the median nerve.
-
Anatomical features A naturally narrower carpal tunnel, which is more common in women, means that even mild swelling can more quickly lead to compression of the median nerve.
What carpal tunnel syndrome looks like clinically
The manifestations of carpal tunnel syndrome are determined by which areas of the hand and fingers are served by the median nerve and by the conditions under which it is compressed. Symptoms develop gradually and have a typical, recognizable distribution.
The main sign is numbness and tingling in the thumb, index, and middle fingers, as well as in part of the ring finger. The little finger is not involved, which has diagnostic significance.
Worsening of symptoms at night or in the early morning is typical. During sleep, the wrist often involuntarily flexes or hyperextends and may remain in this position for a long time. As a result, pressure within the carpal tunnel increases, and the person wakes up because of numbness, tingling, or the need to “shake out” the hand.
Symptoms often depend on wrist position and the type of load. They intensify with prolonged computer work, smartphone use, holding tools, and performing repetitive movements. What matters here is not the intensity, but the duration and static nature of the load.
At early stages, sensory disturbances predominate. As compression persists, signs of involvement of motor fibers may appear: reduced grip strength, clumsiness of movements, and difficulty performing fine, precise actions.
With prolonged compression, there may be a reduction in muscle bulk at the base of the thumb (thenar eminence atrophy), indicating more advanced and long-standing involvement of the median nerve.
The appearance of persistent weakness indicates more prolonged and deeper nerve compression and signifies a reduced potential for reversibility of the process.
Which symptoms are often mistaken for carpal tunnel syndrome, but are not
Pain, numbness, and weakness in the hand can occur in various conditions. Not all symptoms involving the hand are related to compression of the median nerve at the wrist level. Errors most often arise when the location of symptoms is mistaken for their source.
When the problem is located above the wrist
When structures above the level of the hand are affected, symptoms may spread into the arm and fingers, creating the impression of carpal tunnel syndrome, although the mechanism of disturbance is different.
- Problems in the cervical spine. Radiculopathy at the C5-C7 level can cause pain, numbness, and weakness in the arm and hand. In this case, symptoms often extend above the wrist, intensify with neck movements, and are combined with pain in the shoulder, shoulder blade, or neck region. Such a distribution of complaints is not characteristic of isolated compression of the median nerve in the carpal tunnel.
- Thoracic Outlet Syndrome (TOS). In thoracic outlet syndrome, the neurovascular bundle is compressed between the neck and the shoulder. Numbness of the entire arm or отдельных fingers, a feeling of a “heavy arm,” and coldness occur. Symptoms intensify when the arms are raised, during overhead work, and with prolonged static load on the shoulder girdle. Because the hand is involved, this condition is often mistakenly taken for carpal tunnel syndrome.
When nerve compression occurs outside the carpal tunnel
The median nerve and other peripheral nerves can be compressed in other anatomical areas, leading to a similar but fundamentally different clinical picture.
- Compression of the median nerve at the forearm level (Pronator Teres Syndrome).
When the median nerve is compressed above the wrist, in the area of the pronator muscles of the forearm, pain and fatigue in the forearm predominate. Symptoms worsen with wrist rotation and physical load. A characteristic difference is that nocturnal symptoms typical of carpal tunnel syndrome are often absent.
Compressions of other peripheral nerves
- In cubital tunnel syndrome, the ulnar nerve is affected, which manifests as numbness of the little finger and part of the ring finger.
- Compression of the radial nerve causes pain along the dorsal surface of the hand and forearm.
In these cases, the distribution of symptoms does not correspond to the area served by the median nerve and is not related to the carpal tunnel.
When the source of symptoms is not nerve compression
Some conditions cause pain or discomfort in the hand but are not accompanied by the typical signs of compressive neuropathy.
- Tendinitis and tendon inflammation. Tendon inflammation manifests as localized pain that intensifies with movement. Typical numbness, nocturnal awakenings, and the sensation of a “foreign hand” are absent. Such conditions are more often associated with overload, sports, or repetitive physical work.
When the nervous system as a whole is affected
In systemic damage to nervous tissue, symptoms extend beyond a single anatomical canal.
- Generalized neuropathies. Diabetic, deficiency-related, or toxic neuropathy (including heavy metals, pesticides, organic solvents, and other industrial chemicals, as well as alcohol) can cause numbness and tingling in the hands. These conditions are characterized by symmetry of symptoms and simultaneous involvement of the hands and feet. Carpal tunnel syndrome may be present secondarily but is not the primary cause of the complaints.
- Systemic neurological diseases. In conditions affecting the central nervous system, including multiple sclerosis, sensory disturbances extend beyond the territory of a single nerve and are accompanied by other neurological symptoms. Such a clinical picture does not correspond to isolated carpal tunnel syndrome.
- Exposure to mold and mycotoxins. Systemic neuroinflammation and toxic damage to peripheral nerves can mimic compression syndromes, including numbness and tingling in the hands. In these cases, local treatment of the wrist does not eliminate the cause of symptoms and does not lead to sustained improvement.
In favor of carpal tunnel syndrome is a combination of numbness and tingling in the area served by the median nerve, worsening of symptoms at night or in the early morning, and a clear association of complaints with wrist position and hand load. The appearance of persistent weakness, reduced grip strength, or clumsiness of movements is a sign of deeper compression and a reason not to delay further diagnostic evaluation.
How carpal tunnel syndrome is confirmed in real clinical practice
Carpal tunnel syndrome is not confirmed by a single test and is not “visible” through any one isolated parameter. The diagnosis is based on the clinical picture and additional methods, which are used not instead of clinical reasoning, but in support of it.
First of all, the physician focuses on the pattern of symptoms: which fingers become numb, whether nocturnal awakenings occur, and whether sensations worsen with certain wrist positions and repetitive loads. These features alone already allow suspicion of compression of the median nerve.
During the physical examination, simple clinical tests are used in which pressure within the carpal tunnel is artificially increased. If this reproduces the patient’s familiar symptoms-numbness, tingling, or a “shooting” sensation in the characteristic fingers-this supports the mechanical nature of the problem. These tests are not proof on their own, but they work well in the context of a typical clinical presentation.
Electroneuromyography (ENMG) is used to assess nerve conduction. It shows whether signal transmission along the median nerve is slowed and how pronounced the functional impairment is. However, it is important to understand its limitations: at early stages of carpal tunnel syndrome, the study may be normal. This does not mean that there is no problem-it simply means that the changes have not yet reached the level detectable by the instrument. ENMG helps assess the severity of involvement but is not always suitable for early diagnosis, when the process may still be reversible.
Ultrasound examination allows visualization of structural changes. It is used to assess the thickness of the median nerve, the presence of swelling, changes in the shape of the tunnel, and the condition of the tendons. Ultrasound does not show how well the nerve functions, but it helps confirm that it is under conditions of mechanical pressure.
Instrumental methods are especially important when symptoms persist for a long time, worsen, when persistent weakness appears, or when invasive treatment is being considered. In such situations, studies are needed to clarify the picture and to exclude other causes.
The key point is that the diagnosis of carpal tunnel syndrome always remains clinical. Tests and studies do not replace understanding of the mechanism; they only help to уточнить its severity and stage.
Why symptoms do not resolve on their own
Carpal tunnel syndrome does not disappear spontaneously because pressure on the nerve persists. Even if numbness or pain temporarily decreases, the conditions under which the median nerve functions usually remain unchanged.
Within the carpal tunnel, swelling and elevated tissue pressure do not resolve automatically. The tendons remain under tension, fluid outflow stays impaired, and the space of the tunnel does not increase. As a result, the nerve does not receive the period necessary for restoration of blood supply and conduction.
It is important to distinguish temporary relief from true recovery. Symptoms may lessen due to fluctuations in swelling, changes in sensitivity, or reduced load on a particular day. This creates a sense of improvement, but the compression itself persists.
Nerve tissue recovers slowly and only when there is sufficient time without pressure. If the load continues, even at a lower level, the nerve does not have time to regenerate. Therefore, symptoms often occur in waves: they decrease, then return, and over time become more persistent.
When a conservative approach is possible, and when it is not
Management of carpal tunnel syndrome depends not on the mere presence of numbness, but on the condition of the nerve and how long it has been under pressure. As long as compression has not led to permanent damage of nerve fibers, the nerve retains the ability to recover.
In the early stages, sensory symptoms predominate: numbness, tingling, nocturnal discomfort, and a feeling of clumsiness in the hand. Strength may be preserved or decrease only episodically. In such situations, the main problem is not “destruction” of the nerve, but the conditions in which it operates. If pressure can be reduced and the nerve given time without compression, recovery is possible.
The situation changes when compression persists for a long time. Gradually, not only sensory but also motor fibers are affected. Persistent weakness appears, grip strength decreases, and movements become less precise. This indicates that the nerve has already begun to lose functional fibers and that the potential for reversibility is diminishing.
The time factor is also important. Even moderate symptoms that persist for months and do not change despite attempts to reduce load may indicate established chronic compression. In such cases, waiting for symptoms to “go away on their own” increases the risk that changes will become irreversible.
The boundary between conservative and invasive approaches is determined not by the intensity of pain, but by the depth of nerve involvement and the dynamics of symptoms. If sensory disturbances gradually give way to persistent motor deficits, further delay in assessment and decision-making becomes dangerous for hand function.
The role of nutrient deficiencies
Nutrient deficiencies are not, by themselves, the cause of carpal tunnel syndrome. They do not create the carpal tunnel and do not compress the nerve. However, they significantly influence how the nerve tolerates pressure and whether it is able to recover once compression has already occurred.
Vitamin B6 plays a key role in the function of peripheral nerves. It is necessary for normal signal transmission along nerve fibers and for maintaining the nerve’s resistance to stress. With B6 deficiency, the nerve becomes more “sensitive”: it tolerates mechanical pressure worse and develops symptoms more quickly-numbness, tingling, and burning.
Importantly, B6 deficiency does not always mean low values on laboratory tests. In some people, the requirement for this vitamin is higher than average due to metabolic characteristics. In such cases, standard doses may be insufficient, even if levels formally fall within the reference range. This explains why, under similar hand loads, carpal tunnel syndrome develops and persists more readily in some individuals than in others.
For this reason, B6 often appears in clinical observations of compressive neuropathies: it does not eliminate pressure, but it affects how resistant the nerve is to compression and how pronounced the symptoms are.
Magnesium affects not so much the nerve itself as the condition of the surrounding tissues. It participates in muscle relaxation and in reducing excessive tendon tension. When magnesium is deficient, chronic tension of soft tissues develops, tendons relax less effectively, and pressure within the carpal tunnel is maintained longer and more persistently.
In practice, magnesium and vitamin B6 are often considered together because they act on different aspects of the same problem: B6 on nerve conduction and nerve resilience; magnesium on tissue tension and the conditions within the tunnel.
Vitamin B12 is necessary for maintaining the structure of nerve fibers and for recovery processes. When it is deficient, nerve recovery is slower, and symptoms become more persistent and less reversible.
If compression persists for a long time, B12 deficiency can further reduce the chances of full recovery of sensation and strength.
Other B vitamins. Vitamins B1, B2, and folate also participate in energy supply and recovery of nervous tissue. Their deficiency does not directly cause carpal tunnel syndrome, but it makes the course of the process more severe and prolonged, especially against the background of existing nerve compression.
Iron is necessary for normal oxygen delivery to tissues, including nerve tissue. With iron deficiency, the nerve tolerates compression worse and recovers more slowly. Even without overt anemia, reduced tissue oxygenation can intensify neuropathic sensations and slow recovery.
Vitamin D primarily affects the pain and sensory component. With deficiency, pain, burning, and tingling are more likely to intensify. Correction of deficiency does not eliminate mechanical compression of the nerve, but it may reduce the subjective severity of symptoms in the presence of ongoing compression.
Why surgery is not the first step
Surgery for carpal tunnel syndrome is aimed at mechanically reducing pressure within the carpal tunnel by cutting the transverse carpal ligament. This does indeed increase the space available for the median nerve, but it does not eliminate the factors that led to the development of compression in the first place. Tissue swelling, chronic overload, systemic factors, and the conditions that maintain elevated pressure do not disappear after surgery.
It is important to understand that surgical intervention does not automatically restore the nerve. If compression has existed for a long time and the nerve has already lost part of its function, anatomical decompression does not always result in full recovery of sensation and strength. This is why, in some patients, numbness, tingling, or reduced hand endurance persist even after a technically successful operation.
In addition, cutting the transverse carpal ligament irreversibly changes the biomechanics of the wrist. This may affect stability, grip strength, and coordination of fine movements, and such consequences may not become apparent immediately. For the patient, this means that surgery is not a “neutral” intervention, but a step with long-term consequences.
Therefore, a surgical approach is considered when the potential for conservative recovery has been exhausted or when further waiting threatens irreversible loss of function. In all other cases, it is more reasonable to first attempt to eliminate the conditions that maintain pressure on the nerve and to give it a chance to recover without anatomical changes.
What can provide decompression without surgery
Decompression of the carpal tunnel is possible without surgical intervention provided that conditions are created for a gradual and sustained reduction of pressure on the median nerve. This is not about a single method, but about a combination of measures aimed at eliminating both mechanical and systemic factors of compression.
Work with soft tissues, including manual and osteopathic approaches, helps reduce excessive tension in the wrist, forearm, and proximal segments of the upper limb. Restoring tissue mobility improves blood flow and fluid drainage, which contributes to a reduction in pressure within the carpal tunnel without direct impact on the nerve.
The use of a nighttime brace is intended to keep the wrist in a neutral position during sleep. This prevents prolonged wrist flexion that may persist for many hours and eliminates one of the key causes of nocturnal compression. As a result, the severity of nighttime and early morning symptoms decreases.
Correction of nutrient deficiencies creates metabolic conditions for recovery of nerve tissue. Adequate provision of B vitamins, magnesium, and iron increases the nerve’s resistance to compression and supports restorative processes against the background of reduced pressure.
Reduction of swelling and tissue pressure is achieved by limiting provoking loads, normalizing metabolic processes, and decreasing systemic inflammation. Taken together, these measures make it possible to achieve decompression without irreversible anatomical changes in the wrist area.
What really needs to be done during the recovery phase
At the recovery stage, the decisive factor is stopping the influence of factors that continue to damage the nerve. Carpal tunnel syndrome does not recover in parallel with ongoing load-the nerve tissue requires time and the absence of compression.
The key condition is a temporary and complete cessation of provoking activities. This does not mean reducing intensity or doing the actions “less often,” but fully excluding the movements and positions that caused or intensified symptoms. As long as compression persists, even to a minimal degree, nerve recovery is impossible.
Recovery of nerve tissue occurs slowly and in stages and may be accompanied by fluctuations in symptoms. This is an expected process. Attempts to focus on rapid results or to regularly “test” whether it is already possible to return to load most often lead to symptom recurrence and loss of the achieved improvement.
How to prevent recurrence
Prevention of carpal tunnel syndrome exacerbations is based not on treatment, but on changing the conditions under which the hand and the nerve function. After symptoms resolve, it is precisely these conditions that determine the risk of recurrence.
Changing movement habits involves avoiding constant wrist flexion and extension, the habit of excessive gripping of tools, or maintaining unnecessary tension in the hand. Maintaining a neutral hand position and taking regular breaks help reduce baseline pressure within the carpal tunnel.
Even after complete disappearance of symptoms, it is important to limit repetitive loads. Returning to the previous volume of repetitive movements often leads to rapid relapse. Load should remain dosed, taking into account the response of the hand and the time required for recovery.
Early response to the first signs of dysfunction helps prevent recurrent compression. The appearance of numbness, tingling, or nocturnal discomfort is a reason to immediately reduce load and reassess activity, rather than waiting until symptoms become pronounced and persistent.
Conclusion
Carpal tunnel syndrome is the result of prolonged compression of the median nerve within the carpal tunnel, not inflammation or a single episode of overuse. The underlying mechanism is chronic elevation of pressure that disrupts nerve blood supply and conduction, which is why the hand may appear externally normal despite progressive symptoms.
The condition develops under a combination of factors, including repetitive and static loads, soft-tissue swelling, fluid retention, and systemic metabolic background. Load more often acts as a trigger rather than the sole cause. Symptoms progress gradually-from sensory disturbances to motor impairment-and temporary relief does not equal recovery if compression persists. Outcome depends on timely reduction of pressure and elimination of the conditions that maintain nerve compression.