NAFLD: The Largest Hidden Consequence of Chronic Insulin Resistance
Diagnosis “fatty liver” is now increasingly detected incidentally-during ultrasound, CT, or MRI examinations performed for other reasons. It is found in people of different ages, body types, and lifestyles, often in the complete absence of pain, pronounced complaints, or abnormalities in standard blood tests.
Because of this, the diagnosis is often perceived as something insignificant: “many people have it,” “nothing is bothering me,” “the tests are normal.” In medical practice, fatty liver frequently turns into a formal note in a medical report that creates no sense of a real problem for either the patient or the physician.
This article is not intended to frighten with the diagnosis, but to consistently explain what the finding “fatty liver” means, what exactly is happening in the body, why this condition arises, how it can develop over time, and in which cases the changes can be reversed.
What The Diagnosis “Fatty Liver” Means
The diagnosis “fatty liver” means that an excessive amount of fat accumulates in liver cells-hepatocytes, that is, the main working cells of the liver. This refers to fat droplets inside the liver cells themselves, where under normal conditions they are either absent or present in minimal amounts.
In medicine, this term is used as a descriptive one. It records the very fact of fat accumulation in liver tissue, but does not indicate why this occurred, how long the process has existed, or what exactly maintains it. It is a statement of a structural change in the liver, not a diagnosis that explains the cause of the problem.
Here it is important to understand that the liver is not designed to store fat. Under normal conditions, it participates in fat processing, its use for the body’s needs, its temporary binding, and its elimination. When fat begins to be retained inside hepatocytes, this means that the liver has stopped coping with the volume of incoming fat or with the conditions under which it operates, and is forced to accumulate it within its cells.
Why Fatty Liver Is a Consequence, Not an Independent Disease
Fatty liver does not arise on its own and is not a primary disease. It is not an isolated problem of the liver itself but a reflection of processes occurring in the body as a whole. In most cases, fat accumulation in the liver develops as a response to prolonged overload or disruption in the regulation of metabolism.
The liver is the central organ of metabolism. Carbohydrates, fats, and amino acids from food pass through it, as well as hormones, medications, toxins, products of the body’s own metabolism, and substances arriving from the intestine. In essence, the liver functions as a “filter and processing center” that continuously adapts to what and how much passes through it, adjusting the way it operates.
When this load becomes excessive or persists over time, the liver is forced to shift into a compensatory mode—that is, a mode of temporary adaptation. One form of this adaptation is the accumulation of fat inside hepatocytes, the liver cells, when the usual pathways for processing and exporting fat can no longer keep up with the volume of incoming material.
What Happens in the Liver: Mechanism of Fat Accumulation
Under normal conditions, the liver constantly receives fats from different sources. Some come from food, some are released from fat tissue, and some are produced inside the liver itself from carbohydrates when more energy enters the body than it needs. At the same time, the liver processes these fats: it uses them to produce energy, to build cellular structures, or temporarily “packages” them and releases them into the bloodstream so they can be used by other tissues.
In fatty liver, this balance is disrupted. More fat begins to arrive or be produced than the liver is able to process and safely export. As a result, fat remains inside the liver cells—hepatocytes—and gradually accumulates. The cells increase in size, their internal organization changes, and they begin to function less efficiently, especially in terms of energy production and enzyme activity.
It is important to understand that accumulated fat is not neutral or harmless. Its excess makes liver cells more vulnerable to damage, disrupts the function of their energy “stations”—the mitochondria—and creates conditions for the initiation of inflammatory reactions. Over time, this affects the main functions of the liver: detoxification of the blood, protein synthesis, hormonal metabolism, and the normal production and flow of bile.
Thus, fatty liver is not a static or harmless “storage” state. It is a dynamic, evolving process that, if the overloading factors persist, gradually creates the conditions for inflammation and structural changes in liver tissue.
Key Causes Of Fatty Liver Development
Fatty liver almost never forms under the influence of a single factor. In most cases, it is the result of a combination of several causes that chronically overload metabolism and regulatory systems. In different people, the contribution of these factors varies, but the general mechanism is the same: the liver works for a long time under conditions of excessive substrate influx and is forced to change its mode of operation.
Excess weight and obesity. Excess body weight, especially when body mass index is above normal, creates a background metabolic overload. Increased body mass raises the influx of fatty acids into the liver, reduces tissue sensitivity to insulin, and disrupts lipid metabolism regulation. Of greatest importance is visceral fat, which actively releases fatty acids into the portal circulation, even in the absence of obvious generalized obesity.
Abdominal (visceral) obesity. The accumulation of visceral fat is an independent and frequent factor of liver overload. Fat from the abdominal depot actively enters the portal circulation and directly increases the flow of fatty acids to the liver. Importantly, this mechanism can operate even with normal blood glucose levels and without overt general obesity.
Chronic carbohydrate overload. Modern diets are characterized by the constant presence of easily digestible carbohydrates-sugar, baked goods, grains, juices, sweet beverages, and frequent snacking. Even with moderate portions, this dietary structure creates a chronic energy surplus. Under these conditions, the liver regularly encounters an excess of substances from which fat is synthesized and, in the absence of periods of unloading, increasingly directs this excess toward fat accumulation.
Excessive fructose intake. Fructose occupies a special place among carbohydrates because it is almost entirely metabolized in the liver and is readily incorporated into fatty acid synthesis, bypassing many regulatory mechanisms. The main sources are fruits and fruit juices, dried fruits, honey, syrups, and products with “natural” sweeteners. With regular excess fructose intake, the load on the liver can be significant even with normal blood glucose levels and in the absence of overeating.
Insulin resistance and chronic hyperinsulinemia. Insulin resistance usually develops against the background of prolonged carbohydrate overload. Cells respond less effectively to insulin, and the body is forced to maintain elevated insulin levels. For the liver, this means a constant signal to accumulate fat: fat synthesis is enhanced, utilization is inhibited, and export is impaired. This process can persist for a long time with normal blood test results, creating the illusion of metabolic well-being.
Prediabetes and type 2 diabetes mellitus. These conditions reflect clinically significant disturbances in carbohydrate regulation and, as a rule, are accompanied by chronic insulin overload of the liver. The presence of prediabetes or diabetes significantly increases the risk of the formation and progression of fatty infiltration, even with moderate dietary intake.
Anabolic steroids are hormonal substances typically used outside of medical indications to increase muscle mass and athletic performance. They can be an independent cause of fatty liver infiltration. Their effects are not limited to indirect metabolic mechanisms and may lead to fat accumulation in the liver. The mechanism includes direct toxic effects on hepatocytes, mitochondrial dysfunction, and impaired export of fat from the liver.
Dyslipidemia. Elevated triglycerides and reduced HDL levels reflect disturbances in fat metabolism and transport. Under such conditions, the liver becomes overloaded with lipids not only due to increased synthesis, but also due to impaired distribution and export of fat, which contributes to its intrahepatic accumulation.
Choline deficiency and impaired fat export from the liver. Even with active fat synthesis, the liver should not accumulate fat. This requires mechanisms for packaging and exporting fat from liver cells, which depend, among other things, on adequate choline intake. When choline is deficient, fat is produced but retained within liver cells, which can occur even with moderate dietary intake and in the absence of obesity.
Impaired bile flow. Bile plays a key role in fat metabolism and its removal from the liver. With chronic impairment of bile flow, fats and their metabolic products are retained in liver tissue, increasing hepatic overload. Bile stasis may be associated with functional disorders, changes in bile properties, spasm of the bile ducts, or the consequences of inflammatory processes.
Iron overload. Iron is essential for normal physiological function, but in excess it becomes a source of tissue damage. The liver is the primary organ of iron storage and is particularly sensitive to overload. Excess iron enhances cellular damage and increases the toxicity of accumulated fat, accelerating disease progression.
Drug-related and toxic factors. Many medications and toxic substances are metabolized in the liver. With long-term use or the combination of multiple factors, detoxification systems become overloaded, and fatty infiltration may develop as a consequence of such exposure or exacerbate existing changes.
Infectious and parasitic factors. Chronic infections and parasitic processes can exert long-term effects on the liver directly or through systemic inflammation. They may impair bile flow and metabolic processes in the liver, but in most cases they are not the leading cause, rather an accompanying factor of overload.
Rapid weight loss and restrictive diets. With abrupt caloric restriction and rapid weight loss, large amounts of fat enter the liver from adipose tissue. In the presence of protein or choline deficiency, or impaired bile flow, the liver may not be able to cope with this flux, which can lead to temporary or persistent fat accumulation.
Genetic predisposition. Genetic factors are not an independent cause, but they determine the individual threshold of liver resilience to overload. Under the same conditions, changes remain minimal in some individuals, while in others they develop more rapidly and are more pronounced.
Additional Factors That May Contribute to the Development of Fatty Liver
- Age-related metabolic changes in which hepatic metabolic flexibility decreases;
- Age-related hormonal changes, including reduced estrogen levels in postmenopause and androgen shifts in men;
- A sedentary lifestyle reduces glucose and fatty acid utilization in peripheral tissues and enhances their redistribution to the liver;
- Sleep disturbances and chronic sleep deprivation affecting insulin sensitivity and lipid metabolism;
- Obstructive sleep apnea syndrome, accompanied by episodes of hypoxia and increased oxidative stress;
- Endocrine disorders such as hypothyroidism and polycystic ovary syndrome;
- Chronic stress with prolonged elevated cortisol load;
- Alcohol consumption, even in small amounts, may aggravate fatty infiltration of the liver in the presence of other risk factors;
- Alterations in the composition of the gut microbiota, especially in small intestinal bacterial overgrowth (SIBO).
How The Disease Progresses Over Time
The course of fatty liver disease is generally not acute. In most cases, it is a slow process that can develop over years without pronounced symptoms and remain unnoticed. This gradual progression often creates a false sense of safety and delays timely intervention.
The pattern of progression is determined by the combination of underlying causes, the degree of metabolic overload, the presence of inflammatory factors, and the individual resilience of the liver. As long as the damaging influences persist, changes accumulate gradually and sequentially.
Prolonged asymptomatic course. In the early stages, fatty infiltration usually does not produce specific symptoms. Pain is absent, and signs of liver failure are not apparent. Nonspecific manifestations may occur-such as increased fatigue, heaviness after meals, and reduced exercise tolerance-but they are rarely associated with liver problems. Laboratory values may remain within the normal range or show only minor deviations. Despite increasing intracellular overload, the liver continues to perform its main functions.
Gradual accumulation of damage. If the causes of fatty infiltration are not eliminated, the process does not remain stable. Against the background of chronic excess fat, damaging reactions gradually intensify, the function of cellular energy systems is disrupted, and inflammatory mechanisms are activated. The insidious nature of this stage lies in the fact that outwardly the condition may appear relatively favorable, while liver tissue increasingly loses its capacity for full recovery. Damage accumulates slowly but forms the basis for further disease progression.
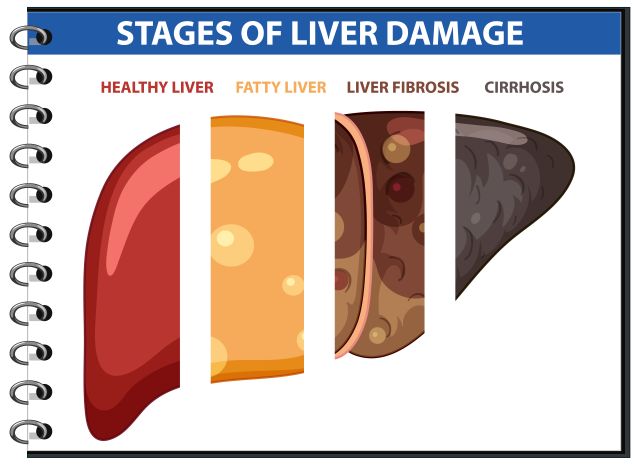
How Fatty Liver Progresses
Although this article focuses on the nonalcoholic form of fatty liver disease, it is important to understand that the same stages-from simple steatosis to cirrhosis-are also characteristic of alcohol-related liver injury. Alcohol abuse remains one of the most significant factors of liver damage, and in clinical practice mixed forms are frequently observed, in which alcohol exacerbates existing nonalcoholic infiltration or accelerates its progression.
Simple steatosis is the accumulation of fat within liver cells without pronounced inflammation and without significant tissue damage. At this stage, liver cells remain viable, the overall structure of the organ is preserved, and the changes are potentially fully reversible. It is at this stage that fatty liver is most often detected incidentally. Well-being usually remains satisfactory, and laboratory tests are normal or borderline. This is the period when eliminating the underlying causes yields the fastest and most pronounced effect.
Steatohepatitis-if the overload persists, inflammation joins fat accumulation. Steatohepatitis develops, a condition in which damage to liver cells is accompanied by activation of inflammatory and immune processes. At this stage, elevations in liver enzymes, marked fatigue, and a feeling of discomfort or heaviness in the right upper quadrant may appear. The disease ceases to be completely “silent,” although symptoms may still be mild. Reversibility remains possible but requires more targeted and consistent intervention.
Fibrosis-with prolonged inflammation, the liver activates a protective response, attempting to isolate areas of damage. Connective tissue begins to accumulate, and fibrosis forms-the gradual replacement of normal liver tissue with scar tissue. Fibrosis reflects the chronic nature of the process. In the early stages it is still partially reversible; however, as it progresses, liver elasticity decreases and functional capacity worsens. Even with relatively stable well-being, overall risks to the body begin to increase.
Cirrhosis is the final stage of disease progression. The structure of the liver is severely disrupted, normal blood flow is altered, and a significant portion of functional tissue is replaced by connective tissue. The capacity for recovery at this stage is sharply limited. It is important to understand that cirrhosis develops not only with alcohol-related liver disease or viral hepatitis. Long-standing nonalcoholic fatty liver disease is one of the real causes of cirrhosis in modern clinical practice.
Diagnosis Of Fatty Liver
In routine practice, fatty liver is most often detected by liver ultrasound, frequently performed for other reasons. Imaging is what allows visualization of fatty changes in liver tissue.
Blood tests measuring liver enzymes (ALT, AST, sometimes GGT) are not used to diagnose fatty liver. These markers can be elevated for many different reasons and do not, by themselves, indicate the presence of fat in the liver. At the same time, in fatty liver disease, enzyme levels often remain within normal limits, especially in the early stages. Thus, elevated enzymes do not mean fatty liver, and normal enzymes do not exclude it.
It is important to understand that ultrasound also has limitations. It records the very fact that fat is present but does not explain why it appeared or how far the process has progressed. Therefore, the finding of “fatty liver” on ultrasound is not a complete diagnosis of the cause, but only a starting point for understanding the situation.
The main diagnostic error lies in perceiving fatty liver as a final diagnosis. In reality, it is a descriptive finding that may mask another, more significant problem. Until it is clear what led to fat accumulation and which factors continue to sustain the process, conclusions about prognosis and further actions remain superficial.
Principles Of Treatment For Nonalcoholic Fatty Liver Disease
Treatment of nonalcoholic fatty liver disease is not related to attempts to “support,” “cleanse,” or “heal” the liver as an organ. This logic is familiar but does not correctly reflect the essence of the process. The liver does not need cleansing: under normal conditions, it independently performs functions of processing and elimination of substances and has a high capacity for recovery.
Nonalcoholic fatty liver disease develops because the liver functions for a long time under conditions of metabolic overload. Therefore, the meaning of treatment lies not in acting on the liver itself, but in eliminating the factors that force it to accumulate fat. As long as this overload persists, any attempts to “help the liver” do not produce a sustainable result.
Fat in the liver is a consequence, not an independent target of treatment. Ultrasound and other imaging methods record changes that have already occurred but do not explain their cause. Attempts to “remove fat” without eliminating the cause lead either to no effect or to temporary improvements followed by a return of changes.
To restore the liver, it is necessary to reduce or eliminate the factors that directly maintain its overload. In practice, this most often means correcting excessive carbohydrate intake, primarily easily digestible carbohydrates. Despite the nonalcoholic nature of the disease, even small amounts of alcohol can slow liver recovery and increase metabolic load; therefore, during the recovery phase it is usually excluded.
When the overloading influence is eliminated, liver recovery occurs naturally. Liver enzyme levels often begin to decrease within weeks, and the structure of liver tissue is restored gradually over months. This is not the result of a single pill or procedure, but a normal response of the organ to reduced load.
There is no universal drug or supplement capable of “curing” nonalcoholic fatty liver disease on its own. However, pharmacological or other treatment may lead to liver recovery in cases where it eliminates a specific causal factor-infectious, parasitic, or drug-induced. In these situations, recovery is a consequence of removing the cause, not the result of “cleansing” or stimulating the liver.
If overload factors persist, neither medications, nor herbal preparations, nor so-called “detoxes” are able to compensate for ongoing metabolic damage. Supportive measures may have value only in the context of eliminating the cause and should not be regarded as independent treatment.
Nutrition And Supportive Measures In Fatty Liver Disease
Dietary correction and the use of supplements are not independent treatments for fatty liver disease and do not replace addressing the underlying cause of its development. The main goal of these measures is to reduce the current metabolic load on the liver and create conditions under which it is able to recover after elimination of the primary damaging factor.
Nutrition in fatty liver disease is not aimed at “burning fat in the liver” and does not function as a universal therapy. Its role is to stop the daily support of the mechanisms that lead to fat accumulation. In practical terms, the greatest importance lies in reducing carbohydrate and fructose load, primarily by eliminating sugar, juices, sweet beverages, excessive fruit consumption, and constant snacking. What matters is not so much total caloric intake as the nature of incoming substrates and the frequency of meals, since these factors determine the insulin and lipogenic load on the liver.
An equally important factor is adequate protein intake. Protein is necessary for the restoration of hepatocyte structure, the synthesis of enzyme systems, and the normal functioning of detoxification mechanisms. Protein deficiency reduces the liver’s capacity for regeneration even after elimination of the main cause of fatty infiltration.
Any supplements may be considered only as supportive measures and only in the context of addressing the underlying cause. In a limited number of situations, substances directly involved in hepatic fat metabolism or influencing inflammatory load may be reasonable, such as choline and phospholipids, omega-3 fatty acids, and certain hepatoprotective compounds such as silymarin. Their action is not therapeutic in the strict sense and does not eliminate the mechanism of fat accumulation. They do not work without reducing overload and do not replace causal intervention.
Methods without a clear mechanism of action-“cleanses,” universal detox schemes, isolated use of supplements without dietary changes and without addressing the cause-do not lead to liver recovery. They create the illusion of active intervention but do not change the conditions under which fatty infiltration develops.
Prognosis
In this context, the discussion concerns an early stage of nonalcoholic fatty liver disease in which the changes are reversible. Recovery is possible provided that the cause of liver overload is identified and eliminated. The liver has significant regenerative reserves and is capable of gradual recovery once the damaging factor ceases to act.
It is fundamentally important to understand that irreversible changes form at the stage of liver cirrhosis. However, within the scope of this prognosis, the focus is not on the cirrhotic stage, but on earlier, potentially reversible changes.
The outcome in nonalcoholic fatty liver disease is determined not by the mere presence of fat, but by how long the liver overload has persisted and how early its source has been eliminated. The earlier the damaging factor is removed, the higher the likelihood of restoring liver structure and function.
Conclusion
Nonalcoholic fatty liver disease is not an isolated pathology, but a reflection of prolonged metabolic overload, to which the liver responds by switching into a storage mode. It does not arise suddenly and does not resolve on its own-there is always a combination of causes at its core that must be identified and addressed.
The mere presence of fat in the liver is not a verdict. At early stages, the changes are reversible, and the body has the resources for recovery. However, the longer the damaging influence persists, the higher the risk of progression to inflammation, fibrosis, and loss of liver function.
Therefore, it is critically important not simply to record fatty infiltration as a “finding” on ultrasound, but to interpret what lies behind it, determine the stage of the process, and identify the factors that sustain it. Only this approach makes it possible to choose the correct strategy and prevent the development of serious complications without losing time.